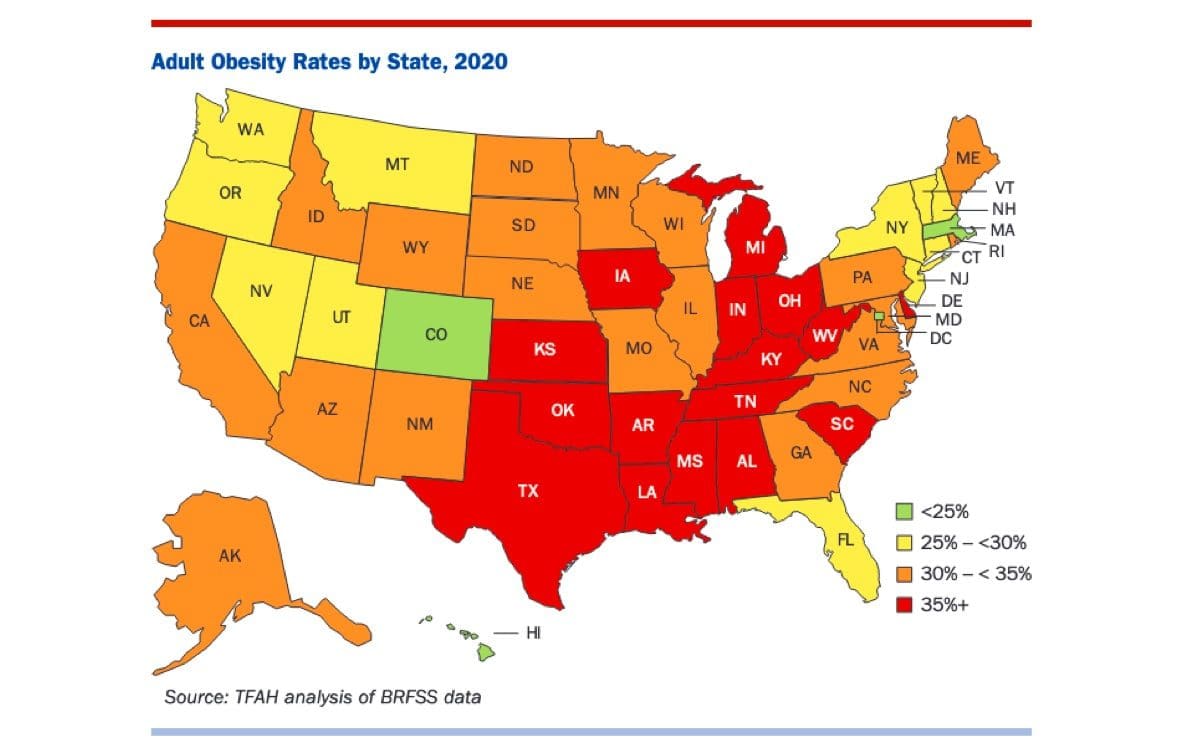
Sixteen U.S. states have an adult obesity rate of at least 35% — a four-state increase from 2019.
This was the key finding in the 18th annual report on obesity from the Trust for America’s Health (TFAH) released in September.
This parallels a World Health Organization (WHO) warning in June that obesity had reached epidemic proportions globally with over 2.8 million obesity-related deaths annually. WHO reports that “most of the world’s population live in countries where overweight and obesity kills more people than underweight.”
Global obesity rates have nearly tripled in recent years. The United States’ adult obesity rate has been climbing since the 1970’s, with the CDC reporting that rates rose from 20.2% in the early 90’s to around 42% by 2018.
Obesity is defined as a Body Mass Index (BMI) of 30 or more. BMI is a ratio of an individual’s weight and height and is one of many indicators of health.
Obesity is associated with higher rates of cholesterol, diabetes, cancer, heart diseases and stroke. These conditions further create complications associated with wound care and infections.
Obesity for women of child-bearing age increases the chance of low birth weight, gestational diabetes, preeclampsia, loss of pregnancy, fetal anomalies, fetal macrosomia and maternal mortality.
Individuals wrestling with obesity experience an increase in mortality and health care costs. Adults with severe obesity (BMI greater than 40) on average have 80% higher medical expenses, and health risks associated with obesity have been compared to the use of tobacco.
Obesity is a complex problem. The common misconception that obesity is simply linked to poor self-control is shallow and short-sighted.
It is true that excess body weight is directly linked to a diet that exceeds the caloric intake needed to sustain a specific individual’s regular physical activity. Yet, this basic equation is frequently complicated by genetic, environmental and economic factors.
Emerging research on income and food scarcity have revealed significant links between income and obesity.
Historic global obesity trends reveal that obesity rates are not the same in every country.
In poor countries, obesity rates increase among the affluent. In middle-income nations, obesity rates tend to be static among all income levels. What is most surprising is that in wealthy nations, the less money a household earns, the higher the rate of obesity.
This trend was confirmed by the Centers for Disease Control and Prevention (CDC). In 2017, the CDC’s National Health and Nutrition Examination Survey found a direct link between income and education and their influence on obesity.
Individuals from households earning less than 130% of the federal poverty threshold saw a rate of obesity around 40%, while households earning over 350% of the poverty level saw rates of 31%.
Income’s influence on obesity is most pronounced in women who see a drop from 45.2% to 29.7% when moving from the lower to higher income brackets.
In like manner, college graduates had less than a 28% obesity rate while individuals with some college or just a high school diploma were 40.6% and 40%, respectively.
So, what is going on here?
In lower-income nations, the problem is that many households do not have access to food or cannot afford sufficient food. The problem in affluent nations is a little more complex.
No one would make the claim that there is not enough food in the U.S., especially since over 108 billion pounds of food is wasted annually. The problem is linked to the kind of food poor households can afford.
Families in or near poverty typically do not earn enough income or receive enough government support to buy the most nutritious foods. While the U.S. has safety net programs to help those in need, a recent report found that 58% of food insecure households encountered one or more obstacles to obtaining such assistance.
Therefore, their grocery carts are filled with food that is high in carbohydrates and not necessarily packed with vitamins and minerals needed to sustain a healthy lifestyle. So, the problem in rich nations is as much about nutritional scarcity as it is about food scarcity.
The assumption that individuals who wrestle with poverty and obesity are lazy is simply wrong. The data reveals that economics is a significant factor.
Many of these households do not get the appropriate amount of vitamins and minerals to sustain a healthy and active lifestyle. Lacking funds to purchase this type of food, they often consume excess calories in the form of carbohydrate-heavy foods in order to ensure the body receives enough nutrients to sustain itself.
Unfortunately, these excess calories ultimately become stored as fat and, over time, a vicious cycle is created that ultimately hails from economic inequality.
Therefore, what can people of faith do? How can we change this process in order to combat this growing trend?
First, we need to change how we view food scarcity. It is not enough to get a meal in a stomach; we need to think about what is being eaten.
The data suggests that people select food based on economics. While school lunch programs, the Women, Infant and Children (WIC) program, and SNAP are all helpful in combating hunger, there is a larger battle to be had related to economic inequality.
Second, we need to encourage and support an economy and infrastructure that not only creates jobs, but also enables families to focus more on nutrition and less on survival. Healthy food should not be a luxury only enjoyed by the rich.
Food and nutritional scarcity, resulting in hunger and obesity, are not the ultimate problems. They are symptoms of generations of social and economic inequality.
- About the Author
- Latest Posts

Chaplain Monty Self is the Director of the Center for Chaplaincy at Charleston Southern University and a board-certified Healthcare Ethics Consultant with the American Society of Bioethics and Humanities.